
Apert Syndrome
Contact the Craniofacial Center
What is Apert syndrome?

Apert syndrome is a rare form of — the early closing of one or more of the soft, fibrous seams between the skull bones (sutures). It is pronounced Ā-pert.
The affects how your baby’s head, face, hands and feet look and work.
Apert syndrome is rare. It happens in about 1 in 80,000 to 160,000 newborns.
In children with Apert syndrome:
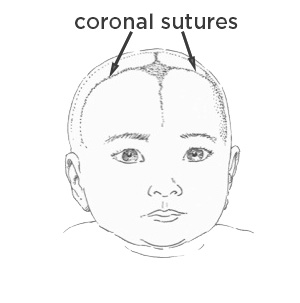
- Both coronal sutures at the top and front of the skull (bicoronal synostosis) close early. These sutures go over the top of the head from ear to ear. (Other sutures, the lambdoid and sagittal, may or may not close early.) Early closure changes the shape of the head and limits room for your baby’s brain to grow. It may increase pressure inside their skull.
- The middle of the face doesn’t develop fully (midface hypoplasia). This will affect how your child’s jaws line up. It can cause problems with chewing and breathing during sleep ().
- Their fingers or toes are joined together or webbed ().
Most children with Apert syndrome have delayed development, though this varies from child to child.
Children with Apert syndrome need coordinated care by providers from many areas of healthcare. At Seattle Children’s Craniofacial Center, our team of experts covers 19 different specialties.
What causes Apert syndrome?
Apert syndrome happens because of a change (variant) in a that affects how bones form. The gene is called FGFR2 (fibroblast growth factor receptor 2).
Most often the condition is caused by a new genetic change that was not inherited from a parent. Other times, a parent passes the FGFR2 gene variant to a child.
The risk of having a child with Apert syndrome is higher if the father is older.
Apert Syndrome Care at Seattle Children's
What are the symptoms of Apert syndrome?
Apert syndrome will likely affect your baby’s head, face, hands and feet.
Head
 Drawn by Raymond Sze
Drawn by Raymond SzeUsually, the sutures let the skull expand as the brain grows. During childhood, the sutures slowly grow together to fully connect the skull bones. The different sutures close at different times. The process continues until adulthood. In Apert syndrome, the coronal sutures (and sometimes other sutures) close early, affecting the skull’s shape.
Babies with Apert syndrome have a skull that tends to be:
- Tall
- Short from front to back
- Wide from side to side
Their forehead is usually flat.
Face
Most often, babies with Apert syndrome have these signs:
- The upper part of their face is flat.
- The middle of their face looks sunken in (concave).
- Their eyes look big and may stick out.
- When their jaws close, the upper jaw is behind the lower jaw (underbite).
As your child grows, their teeth will probably not come together in the front. The small upper jaw will crowd their teeth, causing dental problems.
Hands and feet
Your baby will have webbed fingers and toes. This is a type of syndactyly.
In more severe cases, the thumb is also fused to the fingers. Your child’s hands and feet may look like mittens.
Changes in other parts of the body
- Many children with Apert syndrome have hearing loss.
- Some children with Apert syndrome have a cleft palate (hole in the roof of the mouth).
- Some children with Apert syndrome have problems in the neck (cervical spine).
Less often, there may be small differences in the elbow, bones and muscles or internal organs.
How is Apert syndrome diagnosed?
To diagnose this condition, the doctor will examine your child’s skull carefully. The shape will help the doctor tell if any of the sutures in the skull have fused.
Your child’s facial features will help the doctor tell if they have Apert syndrome or another condition.
Your child may need of their spine, arms, hands, legs and feet to plan treatment. A of the face and skull can give the doctor more information and help us plan the best care for your child.
-
Genetic counseling and testing
Our Craniofacial Genetics Clinic helps identify conditions caused by changes in genes. Our and can help you understand the pros and cons of genetic testing. They can explain test results and your chance of having a child with Apert syndrome in a future pregnancy.
A genetic counselor also will give you information about your child’s condition. Counseling can help you make informed decisions about family planning and your child’s treatment.
Our genetic counselors also advise people with Apert syndrome about their chance of having a child with the condition. A person with this syndrome has a 50% chance in each pregnancy of passing down the gene that causes the condition.
Treating Apert Syndrome
There is no single care plan for Apert syndrome. The treatments and timing we recommend depend on how your child is affected by the syndrome.
Our goal is to minimize the number of steps in the treatment plan by improving the outcome of each step. We want your child to have as normal a life as possible, with plenty of time away from the hospital.
-
Easing breathing
Making sure your child is breathing well is an immediate priority. Differences in the bones in the jaw or midface or an abnormal windpipe can make it hard to breathe.
For children with severe breathing difficulties, they may need a tube inserted in their windpipe (tracheostomy) soon after birth.
Later, your child will likely have surgery to reposition their jaw and face bones to help with breathing and other problems.
Sometimes children have trouble breathing while they sleep (obstructive sleep apnea). Over time, this may lead to problems with how the heart and lungs work. It also can contribute to problems with learning and behavior.
We will ask questions during clinic visits to assess whether this may be a problem. To better understand their breathing patterns, we may monitor your child overnight in our sleep lab (PDF) (Simplified Chinese) (Somali) (Spanish).
The treatment options and timing will depend on your child.
-
Keeping the brain healthy with room to gro
At about 6 months, some babies with Apert syndrome need surgery to reshape the skull and give the brain more room. The procedure is called a posterior cranial vault distraction.
A craniofacial plastic surgeon and neurosurgeon work as a team in the operating room to reshape your child’s skull and protect their brain. The treatment combines surgery to cut the skull bones, followed by distraction osteogenesis to make the skull larger so there’s enough room for the brain.
Some children have posterior cranial vault expansion instead. This is another way to give their brain more room to grow. It does not involve distraction osteogenesis.
Your child’s team will check for signs of fluid buildup (hydrocephalus) and increased pressure in the skull. These problems can happen during infancy or as your child grows.
- If fluid builds up in your child’s brain, they may need a tube inserted to drain away extra fluid. The fluid drains into another part of the body, where it can be absorbed.
- At regular checkups, we ask about warning signs of increased pressure, such as headaches or problems with eyesight. If there are concerns, your child may have imaging scans or a special eye exam to check for swelling at the back of the eye.
-
Protecting the eyes and reshaping the skull
A second operation on the skull brings your child’s eyebrow bone area forward and shortens their high forehead. This allows for continued growth of your child’s brain and helps reshape their skull to look more typical. It also helps protect the eyes.
Our craniofacial plastic surgeon and neurosurgeon work together to perform the fronto-orbital advancement operation.
For a baby with Apert syndrome, we recommend this procedure at 18 months to 2 years. It is done earlier in children with other cranial conditions.
-
Protecting eyesight
An eye doctor (ophthalmologist) will check your child regularly for problems with their eyesight.
- If your child has very shallow eye sockets, their eyes may stick out (proptosis) and be at greater risk of injury.
- Your child’s eyes may not align in the right way because of the position or shape of the eye sockets. This can affect their vision.
- Increased pressure inside the skull can also cause problems with your child’s eyesight.
- Some children with Apert syndrome cannot close their eyes completely. That can irritate the covering on the front of their eyes (corneas). The condition is called keratitis. To avoid harm to their vision, your child may need surgery before they are 2.
-
Surgery to improve breathing and appearance
When your child is 7 to 10 years old, we do an operation to move your child’s midface forward so they can breathe and chew more easily. It improves how their face looks, especially when viewed from the front. The operation also protects their eyes. It is called segmental subcranial distraction.
Our team developed segmental subcranial distraction to treat symptoms and appearance more effectively than the traditional approach (Le Fort III midface advancement). Our Craniofacial Center is the first to use this method. Surgeons around the world are now adopting it.
Segmental subcranial distraction moves bones in the midface different amounts and in different directions. It lengthens the central face and nose and levels the eyes. As a result, the proportions of the face are more normal.
In a study published in the journal of the American Society of Plastic Surgeons, our team showed that this procedure is more effective in normalizing facial proportions than the Le Fort III procedure.


BEFORE (Left): The middle of this boy's face did not grow well because of Apert syndrome. His forehead is high and flat. His cheekbones are sunken. His jaws do not fit together right.
AFTER (Right): As a result of segmental subcranial distraction, the boy's cheekbones have been moved forward. His nose, upper jaw and teeth have moved forward and down. His face is longer and looks more typical. His teeth fit together better.
His upper jaw is finished growing, but his lower jaw will keep growing for several years. At maturity, the jaws will be a good fit.
-
Repairing webbed hands and feet
During their first year of life, your baby will likely need surgery to fix problems with their hands.
If your baby’s thumbs are fused to their index fingers, they must be released at about 6 months. The thumb is critical for the hand to work and develop correctly.
Your child will need multiple procedures to release the fingers on both hands. Ideally, all fingers and thumbs are separated by the time your child is 2 years.
Surgery on the feet is only needed in the most severe cases. Examples would be if the joined toes prevented your child’s foot from striking the ground flat or fitting easily into shoes.
-
Developmental assessment and support
Some children with Apert syndrome have normal cognitive development, but developmental delays are common. The amount of delay varies from child to child.
We will follow your child’s development closely. If we find developmental delays, we will refer you to support services so that your child gets help to reach their full potential.
Your craniofacial pediatrician and social worker will work with you to find resources in the community for children with developmental issues.
-
Dental care and bite alignment
Good mouth care (oral hygiene) is important for all children, but especially those with craniofacial disorders. Our team includes a pediatric dentist and orthodontist who specialize in craniofacial conditions.
The dentist will check your child’s general dental health and look to see if their teeth are too crowded. As your child grows, an orthodontist will check how your child’s upper and lower teeth fit together (occlusion).
Learn more about craniofacial orthodontics.
Your child may need:
- Upper teeth removed to relieve crowding because of their small upper jaw.
- Orthodontic braces to expand the roof of their mouth (palate) and align their teeth.
- Braces or appliances to put their teeth in the best position before jaw surgery.
- Surgery to move the upper jaw forward Le Fort I maxillary advancement if their teeth do not fit together well when your child’s face bones have finished growing. Usually, this happens at 16 years for a female and 18 years for a male.
- Braces to hold the teeth after jaw surgery until they settle in their new position.
Why choose Seattle Children’s for Apert syndrome treatment?
Each year, Seattle Children’s Craniofacial Center cares for hundreds of children with craniosynostosis, including rare syndromes like Apert. Our team has more experience caring for children with craniosynostosis than any other center in the United States. We have experts in every field your child might need.
Many of our patients are newly diagnosed babies. We also care for children who received their initial care at another hospital. We treat children, teens and young adults up to age 21 and sometimes beyond.
- The right treatment at the right time: Our experience helps us find problems early and take steps to treat them or prevent them from getting worse. We watch carefully for problems with your child’s breathing, vision and development or other concerns and recommend care for any issues that arise.
- Better results with fewer surgeries: Our approach helps children with Apert syndrome get the most benefit from surgeries early in childhood. As a result, later in life, some surgeries are either not needed or are less extensive.
- Team-based care from experts: We’ll bring together all the team members your child needs, such as a craniofacial ; nurse; ; ; craniofacial ; pediatric ; ; ear, nose and throat specialist (); ; and , among others.
- Support for your whole family: A diagnosis of Apert syndrome can be scary. We take time to explain your child’s condition. We help you understand your child’s treatment options and make the choices that are right for your family. Every family is offered social work support.
- Research to improve care: Our team created a clinical care pathway to guide treatment for craniosynostosis based on research about what is most effective. Our research is helping us to:
- Better understand the genetic causes of craniosynostosis
- Study how the condition affects learning and behavior
- Build a library of 3-D images to better measure the results of surgery and improve treatments
Contact Us
Contact the Craniofacial Center at 206-987-2208 for an appointment, a second opinion or more information.
If you live outside of Washington, Alaska, Montana and Idaho, please contact our coordinator for out-of-area patients at 206-987-0814.
Providers, see how to refer a patient.
Paying for Care
Learn about paying for care at Seattle Children’s, including insurance coverage, billing and financial assistance.