Provider Q&A: Navigating Urgent vs. Emergent Fracture Care
March 5, 2025
 Fractures are a common childhood injury, but determining the best place for your patient to seek care can be confusing because every case is different. We sat down with Dr. Mike Tretiakov, one of our orthopedic surgeons, and Ann Hilmer, one of our orthopedics and emergency medicine nurse practitioners, to discuss options for fracture care, and the tools community providers can access to determine the best place to send their patient.
Fractures are a common childhood injury, but determining the best place for your patient to seek care can be confusing because every case is different. We sat down with Dr. Mike Tretiakov, one of our orthopedic surgeons, and Ann Hilmer, one of our orthopedics and emergency medicine nurse practitioners, to discuss options for fracture care, and the tools community providers can access to determine the best place to send their patient.
Q: Fractures are a pretty routine injury in the pediatric population and those families are most often directed to the ED for treatment. Is the ED typically the most appropriate care setting for a broken bone?
Dr. Tretiakov: Fractures come in many shapes and sizes, with the majority needing to be seen quickly, but not the same day. Most should be seen in clinic because this is the best, safest, most efficient place to manage them. Some must go to the ED, and others are urgent, but not emergent, and can come to our same-day Orthopedic Injury Urgent Care clinic.
Ann: The Emergency Department is absolutely the best and safest place for a child in extremis when there is a concern for an undifferentiated injury, fracture, or infection. It is where the ED providers can perform rapid neurovascular assessment, provide pain control, diagnostic clarification is made, treatment plans are initiated, and follow-up care is established.
It is likely no longer an emergency when a fracture is identified at the PCP office or urgent care. If the initial exam is reassuring against life or limb threatening injuries, pain control has been provided, and the fracture is immobilized, an exam from an ED provider is likely not additive.
Q: How would a PCP or urgent care provider know what fractures indicate a trip to the ED vs. another care setting?
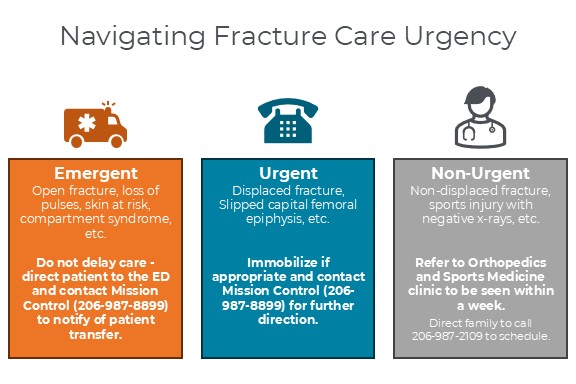
Dr. Tretiakov: First, the provider should check for rare but concerning findings such as nerve or blood vessel injury, skin at risk, or compartment syndrome. While these are very uncommon, they warrant transfer to an ED. Calling us is very helpful, but should not delay care. However, the vast majority of fractures or orthopedic injuries are urgencies, not emergencies. Most fractures can be seen in our clinic within 3-5 days or come to the Orthopedic Injury Urgent Care clinic on a walk-in basis. Sometimes when there is obvious deformity, such as a broken forearm, we may need to do a procedure like a reduction. Many cases are in between, such as mild to moderate displacement. For fractures that you are concerned may need a procedure, feel free to call us so we can help triage appropriately.
Ann: Open fractures or obviously deformed extremities need the ED. Many fractures require urgent, but not emergent, procedures. Depending on several factors, the ED may or may not be the best place for these procedures to be done. We cannot predict the ability of the ED to support procedural sedation, nor can we predict the timing of the Orthopedist to be available for consultation once a family arrives in the ED. For this reason, a call to Mission Control (206-987-8899) or a page through the Provider-to-Provider Line (206-987-7777) can help the community provider navigate when and where the patient should receive the next step of treatment or diagnostics for their orthopedic concern.
Q: What kind of support is available at Seattle Children’s to help providers and families determine the best next steps when dealing with fractures?
Ann: If providers need help determining the best next steps for patient care, there are several resources they can access for guidance:
- Mission Control: If you are seeking orthopedic consultation through the Emergency Department because you believe your patient needs urgent attention (further diagnostics, pain control, procedural sedation, or possible surgery), Mission Control is the best place to start. Mission Control is staffed 24/7 with quick access to a nurse who connects community providers with the appropriate teams – in this case an orthopedic provider who can review imaging and determine a treatment plan over the phone with you. This may mean transfer to the ED for sedated procedure, direct admission to the hospital, referral to Orthopedics and Sports Medicine (clinic or urgent care), or a scheduled procedure in the OR procedure room within the week. Several factors contribute to the best time and place for a patient to receive their care, and Mission Control can help navigate those factors in real-time.
- Urgent Provider-to-Provider Line Call: If you do not believe your patient needs to be seen in the ED for their fracture but believe they require more urgent consultation, you can call the Provider-to-Provider Line with an urgent clinical question and discuss with our on-call orthopedic surgeon.
- Orthopedics and Sports Medicine Clinics: If there is a known fracture, patients do not need a referral from their PCP to be seen in the Orthopedics and Sports Medicine clinic or urgent care for follow up. Families can call or go online to make an appointment themselves. For stable, splinted fractures, families are offered appointments for follow-up and casting within a week. It can help if the PCP or urgent care provider reassures families that the waiting period does not negatively impact healing of the fracture nor increase likelihood of complications.
Q: Mission Control is most often used for ED-to-ED transfers. What are the benefits for a PCP or urgent care provider in calling the team prior to sending a patient to the ED?
Dr. Tretiakov: Calling Mission Control first is very important because it helps us provide the most effective care for patients. For patients who do not need a procedure, such as for a nondisplaced fracture, clinic is the best setting. For those that clearly need a procedure (very broken forearm), there are many options. The ED can provide sedation for reductions, but sometimes when they are very busy sedation is either delayed or not possible. We also offer procedure slots with anesthesia (MAST) and designated ED sedation slots each morning that significantly streamline care and create a better patient experience. If you have a patient who you think needs a procedure, or want to know if a procedure is necessary, its best to call Mission Control so we can help triage the procedure and appropriate resources.
Ann: Orthopedics and emergency medicine are separate services that work together every day to deliver the best care for patients with orthopedic injuries. A phone call to Mission Control can put a provider in consultation with the same orthopedic trauma provider that would care for the patient in the ED, who is in constant, direct communication with the ED providers and nurses that will help deliver care. This team has real-time information related to patient census, wait times, sedation capacity, and ED staffing that can help us determine the best care setting for each patient.
When a call is made beforehand and the patient requires the ED for care, orders can be placed, and care teams can be mobilized in anticipation of the patient arrival. The call can save families hours of waiting for an orthopedic consultation (or the need for an ED visit altogether).
Q: What are the benefits to the family if they can avoid a visit to the ED if there is a more appropriate care setting?
Dr. Tretiakov: There are many benefits apart from the obvious cost savings and avoidance of viral exposure in the ED. Most orthopedic injuries are isolated injuries that are best managed in focused setting like clinic, a procedure room, or operating room where there is a designated time slot and appropriate staff, equipment, and resources to manage that injury. Since few fractures are true emergencies, there are many options to deliver excellent care that is outside the ED.
Ann: At times, the dynamic and ever-fluid patient acuity and volumes in the ED limits our ability to perform non-emergent sedated procedures, which is a frequent and surprising dissatisfier for families. When we communicate in advance, families can be made aware of anticipated wait times or even offered safe alternatives to an ED visit. Additionally, when applicable, Mission Control can also facilitate direct admissions with the orthopedics team for surgeries and initiate discussions with the OR staff before the patient arrives. Our communication together (PCPs and urgent care providers as the pre-hospital team and us as the specialists) significantly improves the quality and efficiency of patient care delivery and is an important way to reduce health care costs for families.
Additional Resources
- Orthopedics and Sports Medicine Refer a Patient Page
- Orthopedic Injury Urgent Care clinic information
- Mission Control: 206-987-8899 or 866-987-8899
- Provider-to-Provider Line (for urgent clinical questions): 206-987-7777
- ED vs. Urgent Care Guide for families